 Last week, I had the honor of speaking at the Louisville Innovation Summit, where the theme was “Creating the Future of Aging Care.” This was my first time visiting Louisville, which is the home base for several large organizations in healthcare and long-term care.
Last week, I had the honor of speaking at the Louisville Innovation Summit, where the theme was “Creating the Future of Aging Care.” This was my first time visiting Louisville, which is the home base for several large organizations in healthcare and long-term care.
Much of the conference was interesting (you can see the program here) but what captured my interest and imagination the most was this: in his keynote, Paul Bennett, the Chief Creative Officer of IDEO, urged the city of Louisville to take the lead in reimagining aging.
Now, in truth I’m not really sure what he has in mind when he says this and I suspect that it’s different than what I think of. To begin with, he explained that IDEO is launching a global project on aging called The Powerful Now. Here’s how the project is described on their site:
“AGING IS BEING REDEFINED.
NOT AS A PATH OF DECLINE, BUT ONE OF RENEWAL.Doesn’t that match your own hopes, wishes, and desires? To become more curious. More engaged. More vibrant. Physically and emotionally. Deeply connected to the ideas and the people who matter to you.
The Powerful Now is about bringing the power of creativity to how we conceive of, design, and experience aging. If you were to add up all the people who are fifty years and older, they would be the third largest economic superpower on Earth.”
Hm. I am all for reimagining aging in positive terms. But what I care most about is solving the age-associated problems that cause older adults and their families the most excess suffering.
What I want to see is a city that creates or implements effective systems for optimizing the health, function, wellbeing, independence, and dignity of older adults. And I want to see a city that succeeds in doing so especially for older adults who are experiencing:
- Medical complexity, meaning multiple chronic illnesses or health problems such that they often encounter the hospital or emergency room
- Chronic impairments of mind, body, or both, meaning dementia or chronic impairments of physical function
- Difficulty managing ADLS and/or IADLs (which is usually due to acute or chronic impairments of body or mind, obviously)
- Residence in assisted-living or a nursing home.
The images we use as we articulate our vision of better aging are important. Paul Bennett spoke of how moved he was by seeing older adults in a Shanghai park, waltzing as they did their group exercise.
Very nice. But I want to see images of people with walkers waltzing. I want more images of people who need support, and yet are still living vibrant lives and contributing to the community around them. You might have mobility impairments and need services and because you are GETTING the services you need, you are able to volunteer and help your community benefit from your wisdom or experience or education or even just presence as a friendly person.
I also want to see a city that effectively helps family caregivers support their older loved ones with the problems above.
Taking on such a project at a city level actually makes a lot of sense. To help older adults live their best lives, even as they face the common challenges of aging, you need to integrate health care, social services, housing, employment policies (esp as regards family caregivers), and much more. Seems to me that a city would be a good laboratory for experimenting or attempting to implement best-known practices. Once one city has made progress, it can serve a model for other cities.
So if Louisville wants to do this, what needs to happen?
I actually know very little about what enables cities to mobilize on a big project like this. But if I were to get going on this, I’d start by making a list of what’s needed, and then I’d look for promising approaches to meet each need. Then I’d work on implementing those approaches and making a plan to assess how well it’s working as you go along, a la Plan-Do-Study-Act method.
(After drafting this post I found that AARP does have a network of “age-friendly cities” and offers a toolkit here. If anyone knows how well that’s been going for those cities, post a comment! And do they ever have conferences related to this project??)
A list of what’s needed and promising approaches would make a good agenda for a future conference.
What’s needed for a city to better support an aging population
1.Assess your older population, along with what they need and want
Probably the first thing to do is start assessing the older people in Louisville. How many are there now, and what kinds of challenges are they facing? I would think that a combination of surveying/data gathering plus focus groups and community forums would bring up a lot of information.
It would be especially nice for neighborhoods and older adults themselves to get involved in this process of identifying what’s needed and brainstorming solutions. My own experience has been that a lot of older adults are pretty pragmatic about what they want and are less interested in gauzy reframings (i.e. rebrandings) of the aging experience. They want help living their lives, and often staying where they are without imposing an undue burden on their families.
New York City is not Louisville, but there is a lot to learn from the ongoing NYTimes series on life for six 85+ year-olds. (See here, here, and here.) The third article in particular focuses on the “fragile patchwork of care” that exists. That patchwork is one of many things that Louisville could work on if they want to take the lead in improving aging care.
In terms of what people need and want, I feel it might make sense to organize it depending on a certain classification of a senior’s needs and health status. Consider the following groups of Medicare beneficiaries, which I described in more detail in this post:
- Seniors with no substantial chronic functional impairments. These are the seniors who are able to live in their homes, and can manage ADLs and most IADLs without the help of another person.
- Within this group, you’ll have those with no chronic conditions, so they mainly need support in healthy and engaged lifestyles. But most have some to many chronic conditions, and so supporting them in managing their symptoms and getting the right maintenance care will be key.
- Seniors with chronic functional impairments. These are the seniors who require regular help or supervision from other people, due to cognitive problems or physical limitations. Caregivers — paid or family — are chronically involved in their life care and health care.
- Could divide these based on level of impairment, or whether they live at home vs in residential facilities.
- Dementias such as Alzheimer’s are common and pose special problems. It might make sense to design solutions specifically for people in this group, and create subgroups based on whether people are in mild, moderate, or severe stages of dementia, along with whether they live at home (home alone or home w others? I’ve taken care of both, very different challenges!) versus in a residential community.
By the way, here is a chart that I included in my ebook, showing the prevalence of functional impairment in older adults; it’s from a Census Bureau report titled “65+ in the United States: 2010.”
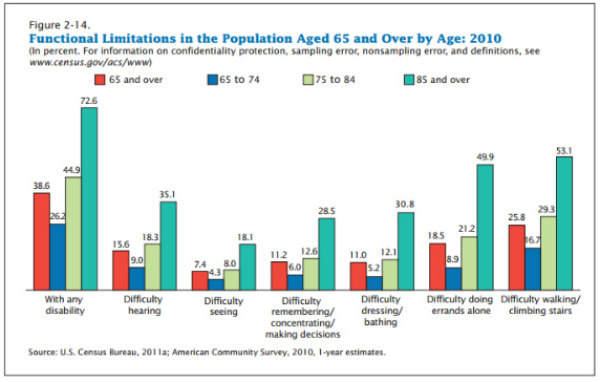
See all those functional impairments? How do you change things within a city, to mitigate those impairments or otherwise help people live their best lives despite having those impairments? That’s what Louisville will hopefully figure out.
Get those people waltzing, volunteering, socializing, and doing things that add meaning to their lives.
Oh and, they almost certainly have other health problems, so you’ll want to help them manage their chronic health problems effectively, and recover from hospitalization or acute health crises effectively. Without crushing their family caregivers with off-loaded medical or custodial care. (I heard they are getting Medicare patients home after surgery much faster. Very nice and saves money on hospital/rehab expenses, but who is helping family caregivers with the extra work??)
2. Identify promising approaches to managing health and life challenges of older adults
Once you’ve identified some main categories of challenges, what are the most promising approaches for meeting them?
Since I’m a doctor who believes that good primary care is key helping patients with what matters most, plus it’s the foundation for high-value healthcare overall, let’s start by considering better primary care approaches.
We do know that older adults who are medically complex struggle to manage their self-healthcare. (See the story of Joan.) It’s important to provide effective assistance, both to reduce any excess suffering of the older person — and their family — and to delay or prevent further declines in health and function.
Fortunately, we already know of some models of healthcare that are proving to be more effective, when it comes to better primary care for seniors. Iora is applying their signature comprehensive primary care approach to seniors in Phoenix and a few other locations. (And look, they are contracted with Humana, which is based in Louisville!) The GRACE model is another approach proven to reduce costs and improve outcomes in high-risk seniors. Still another option is Guided Care. Last but not least, I’m a huge fan of the work being done by geriatrician Joanne Lynn at the Altarum Institute; her team has terrific ideas on re-envisioning a combo of healthcare and long-term supports for older adults.
Sadly, for the truly frail, the wonderful Program of All-Inclusive Care (PACE) model is not an option in Louisville, because they don’t have a PACE program yet. But maybe it’s worth considering?
Of course, it’s not just the high-risk or very frail who should get improved senior health services. Ideally older adults would get better services BEFORE they become high-utilizers. I don’t have time to research it now, but I hope such programs exist. Louisville, find them and bring them to your seniors!
Now what about promising approaches for everything else that older adults need? Some other areas to investigate, for better approaches, would be:
- Management of acute hospitalization and the post-hospitalization period.
- Assistance with IADLs and ADLs for people living in the community.
- Helping people with IADLs — transportation, shopping, meals, home maintenance — is a big part of helping people age in place. ADL support generally takes more work.
- Would be interesting to explore the Village movement and “naturally occurring retirement communities“
- Best practices for senior housing, for assisted living and SNF-level care. Earlier this year the Atlantic ran a very good article titled “Building Better Nursing Homes,” which covers the Green House movement AND the effort to improve existing facilities.
- Supporting people with dementia and their families, whether people are living in their homes or in residential facilities.
- Ways to optimize socialization, activities that provide purpose and meaning, and inter-generational activities.
- Helping an aging population with financial vulnerability, and protecting them from scams.
What would be especially innovative would be to find a way to provide services to people who are low-income AND to those who aren’t poor enough to qualify for Medicaid (but aren’t rich enough to pay for all services needed right now.) Does this mean creating innovative ways to help people pool resources, or to plan ahead for their future aging needs? Who knows, Louisville could help us learn more.
For each type of problem and approach, technology has a role to play. But we should start with the problem first, and then look for tech that helps us solve it.
3. Develop policies and services to support family caregivers
Family caregivers are so important that I am giving them their own special section.
Education and support for family caregivers should, of course, be integrated into healthcare and long-term supports and services.
But if a city wants to take the lead in innovating for aging, it would be fantastic to involve employers in this process. How to do it? AARP’s 2015 on valuing family caregivers includes a number of policy suggestions. Louisville employers could explore these.
4. Better advance planning
I am throwing this in because it’s something that I’ve been thinking a lot about recently.
There’s a town in Wisconsin that made the news in 2014 because a surprisingly large proportion of the population has addressed end-of-life planning.
This is cool, but what is just as important as planning for your death? Planning for your aging.
Specifically, what is hard is planning ahead for a time of prolonged physical or cognitive disability. I think planning for dementia is especially hard, because it’s terrifying for people to consider. However, in my consultation practice, I see a lot of heartache and hassle that has resulted from people not planning for this.
Hope for the best, plan for the likely or quite possible. That’s the advice I give to seniors and their families.
At the very least, people should have set up a durable power of attorney for health and for finances.
Planning ahead also means doing some financial planning, or at least figuring out some options and talking to your family about your preferences. What if, like Katy Butler’s father, you have a stroke and undergo a slow decline over a few years? Would you want a pacemaker? Or would you want your care to focus most on optimizing your function and comfort?
It would be neat if Louisville helped design or pilot or implement a better way to get more people to address this kind of planning.
Do you know of a city implementing this problem-based approach to aging?
I know there’s been a move towards age-friendly cities worldwide. Can anyone share some examples that might be inspiring and useful?
Meanwhile, I hope Louisville goes for this! They have a lot of resources to leverage, and they could do wonderful things for their older population. I hope to hear more about promising approaches to meeting the needs of a city’s older population at a future Louisville Innovation Summit.

Per usual you have a lot of excellent points. so much varies by individual health problems and income.
In my case my problems are minimum. We are financially comfortable and my spouse has stage 4 CKD…but there is a lack of information to help me care for him..no dietition with expertise…little information on what dialysis actually involves, luckily I have a decent nutritional background and am creative. But I tire easily and struggle to do the necessary cooking etc. I am constantly trying to maintain my physical strength and am fearful about being alone as We are not native Milwaukeeans or even Wisconsonites and this is a cliquey town.
Having been involved in health planning (certificate of need, etc) I have tools to look ahead, but I am concerned about the future.
thanks for your interesting and thoughtful communications.
Thanks for your comment.
have you taken a look at the AARP age-friendly cities project? I’m wondering whether that sounds like it would provide you with what you need.
We came to Milwaukee because one of our sons is a pediatrician here. Madison is probably more retiree-friendly and if our son and his wife relocate after he retires I might move there…there is a very good continuing care facility there.
I like the iora program in Phoenix. If there were one here I might consider it…but I enrolled in a standardized Medigap program through Hadassah before we moved from Connecticut and I would lose that. In CT premiums do not increase as you get older as it is community rated. Wisconsin has a waiver from the standardized medigap plans.